
[Note: This is not a story about insects, though it does relate to pest control. As an urban extension entomologist I get to train and work with pest control professionals. These good folks often find themselves called upon to handle and remove a variety of pests, including bats, raccoons and other urban wildlife that can be carriers of rabies. So the following post is adapted from one I recently wrote for the pest management industry, with possible relevance to the readers of this blog.]

“Bonnie and Clyde” are the two stray dogs biting people in my neighborhood. The dog on the left is the one that bit me in August. Both are still on the loose. Uncollared, stray dogs are a rabies and public health risk, and should be reported to animal control. Photo courtesy Plano Animal Services.
Last August I was out for an early morning run when a stray dog rushed me from an alleyway and knocked me down. In light of other dog attacks in Dallas last summer, at least one of which was fatal, I naturally feared the worst as the dog clamped onto my ankle. But as soon as I recovered my wits enough to defend myself, the dog was off. The whole incident probably took no more than five seconds.
Thus began my education about rabies and rabies vaccinations. I’ve known a long time about the seriousness of the rabies virus: how when it takes hold of its victim it is almost certainly fatal; how a victim’s last days are spent in convulsions, wanting and needing water but unable to swallow due to spasms of the voicebox; and how death from respiratory failure usually takes place within 3-5 days of when symptoms begin.
Although my bite was shallow, I knew enough about rabies to realize I shouldn’t ignore it. On the other hand, I wanted to make sure I really needed the shots (I hate shots). I learned within a few days that the same dog had been responsible for biting others in my community, and that the local animal control was working hard to catch it and its partner. I hoped that perhaps the animal would be caught and would test negative. In fact, several days after the attack I spoke to the head of animal control in our town who was very familiar with these criminal dogs. He told me that in his opinion, given their behavior, they were likely not rabid. He explained that almost always a dog that has become infectious will show symptoms of rabies including abnormal behavior, partial paralysis, or lethargy within five days of becoming infectious.
At this point I had a big advantage of knowing someone in the Texas Department of State Health Services. Dr. Shelly Stonecipher, at my local DSHS regional office was very helpful, answering my questions for over an hour, and advising me that the emergency room was probably my best, and most affordable, option. My county health department, I was told, should have the necessary vaccines on hand, but would not take insurance and would have to charge the full wholesale cost of the vaccines. This was my first big shock. The health department cost for the first shot alone would likely be around $2,000. The emergency room would be more expensive, but at least it would be covered by my health insurance.
Dr. Stonecipher explained that post-exposure treatment of rabies is very effective, but to work it needs to be given before symptoms occur (some sources say vaccination should take place within 1-6 days, other sources 10 days or more…a disturbingly loose margin of error). The treatment consists of five shots. The first shot, called the human rabies immune-globulin shot, is given only if a bite has taken place and infection possibly already occurred. The purpose of this shot is to confer rapid, though shorter lived immunity to the rabies vaccine. This was the most uncomfortable of the injections, though not as bad as what I was told rabies shots used to be like (painful injections to the abdomen were the standard treatment up until the 1980s). I was told by my emergency room doctor that at least half of the 10 ml immune-globulin shot is supposed to be administered as close as possible to the site of the bite.
One online source says this shot should be given the day of the bite. However, in my case, no one I talked to in the medical community seemed especially urgent about my getting the shot immediately. I thought I could wait up to 10 days, the quarantine time for some domestic animals. This would, I’d hoped, buy some time for the dog to be caught [It never was caught and is still, six months later, on the loose in my community–our neighbors now refer to them darkly as Bonnie and Clyde]. As it was, I waited eight days; but if I had to do it over I probably would not have waited more than five days.
The next part of treatment is four rabies vaccine shots given in the arm–one the same day as the immune-globulin shot, and the others on days 3, 7 and 14 after the first shot. Rabies vaccine confers longer term immunity via antibodies. But the vaccine may not work quickly enough to prevent rabies if someone has already been bitten by a rabid animal. That’s why these are given in combination with immune-globulin.
The vaccine shots were easy and painless compared to the monster immune-globulin shot. This rabies vaccine series is what anyone wanting pre-exposure rabies prophylaxis would receive. After getting my first immunization at the emergency room, I was told that the most affordable and convenient way to get the rest of the series was through one of the local clinics that specialize in vaccines for travelers. Luckily there was a Passport Health office near my workplace. Also, I discovered that some hospitals carry rabies vaccine shots which you can get by having a prescription from your doctor and making an appointment, thus avoiding the emergency room.
I was surprised by two things regarding my dog attack. First, no one I spoke with seemed to care or really have strong opinions on when or whether to start the course of treatment. My doctor left the choice up to me. Some medical offices seemed not to know a lot about rabies treatment. Websites had conflicting information about virus incubation periods. In other words, I was on my own to figure out what to do about my health.
My second surprise was the cost. Even with insurance, my out-of-pocket cost for the vaccine series alone was close to $1,000. Even more appalling, the following month the bill from the hospital arrived. The overall bill to myself and my insurance provider for an immune-globulin shot, first vaccine, and 15 minutes of an ER doctor’s time, came to $10,179. The itemized bill (which I had to request) listed the immune-globulin shot as the biggest expense, $8,318! According to the hospital, after “discounts” and insurance contributions I personally still owed over $1,800. All this to say, saving your life after a bite from a rabies infected animal is expensive–even with insurance. Estimates of cost of rabies post-exposure treatment on the Internet are highly variable, but my sticker-shock experience does not appear to be unique.
Advice for anyone working with animals
Fortunately, human rabies cases and deaths in the U.S. are relatively rare, averaging 2-3 people a year. This low rate is due to the wide use and effectiveness of the rabies vaccine, but it doesn’t mean that precautions are unnecessary. The CDC recommends that veterinarians and staff, animal control and pest control professionals, spelunkers, and rabies laboratory workers be offered the rabies vaccine. The vaccine should also be considered for any one whose activities bring them into frequent contact with potentially rabid animals, and for international travelers who might come in contact with rabid animals (treatment may not be readily accessible in all foreign areas).
My ten pieces of advice for anyone concerned about rabies:
- If bitten by a stray animal or any wildlife known to be a potential rabies carrier, don’t ignore the bite. Talk to your personal or ER doctor to assess your risk, and determine whether you need treatment for rabies. Wash the wound site from any animal bite as soon as you can with soapy water and iodine based disinfectant.
- If possible, take steps to have the offending animal, like a bat, captured for testing. It could help you avoid expensive post-exposure prophylaxis. Care should be taken not to damage the head of the captured animal, as this may prevent laboratory testing for rabies. Your doctor or veterinarian, or in Texas any of the Department of State Health Services regional offices, can assist with instructions on how to submit an animal for testing.
- Don’t attempt to feed wildlife or touch any stray or feral animal. Use proper protective gear, including double plastic bags, when picking up dead animals.
- Make sure your own pets and livestock, including horses, dogs, cats and ferrets, are up-to-date on their rabies vaccines.
- If you work under conditions that bring you into close contact with bat roosts, do bat removal, or do urban wildlife control, getting the pre-exposure rabies vaccination series is highly recommended. It is much cheaper and easier than post-exposure treatment.
- Even if you are pre-vaccinated, you may still require a series of two post-exposure vaccine boosters after a bite from a possibly rabid animal. This is still much cheaper than post-exposure treatment. Check with your doctor.
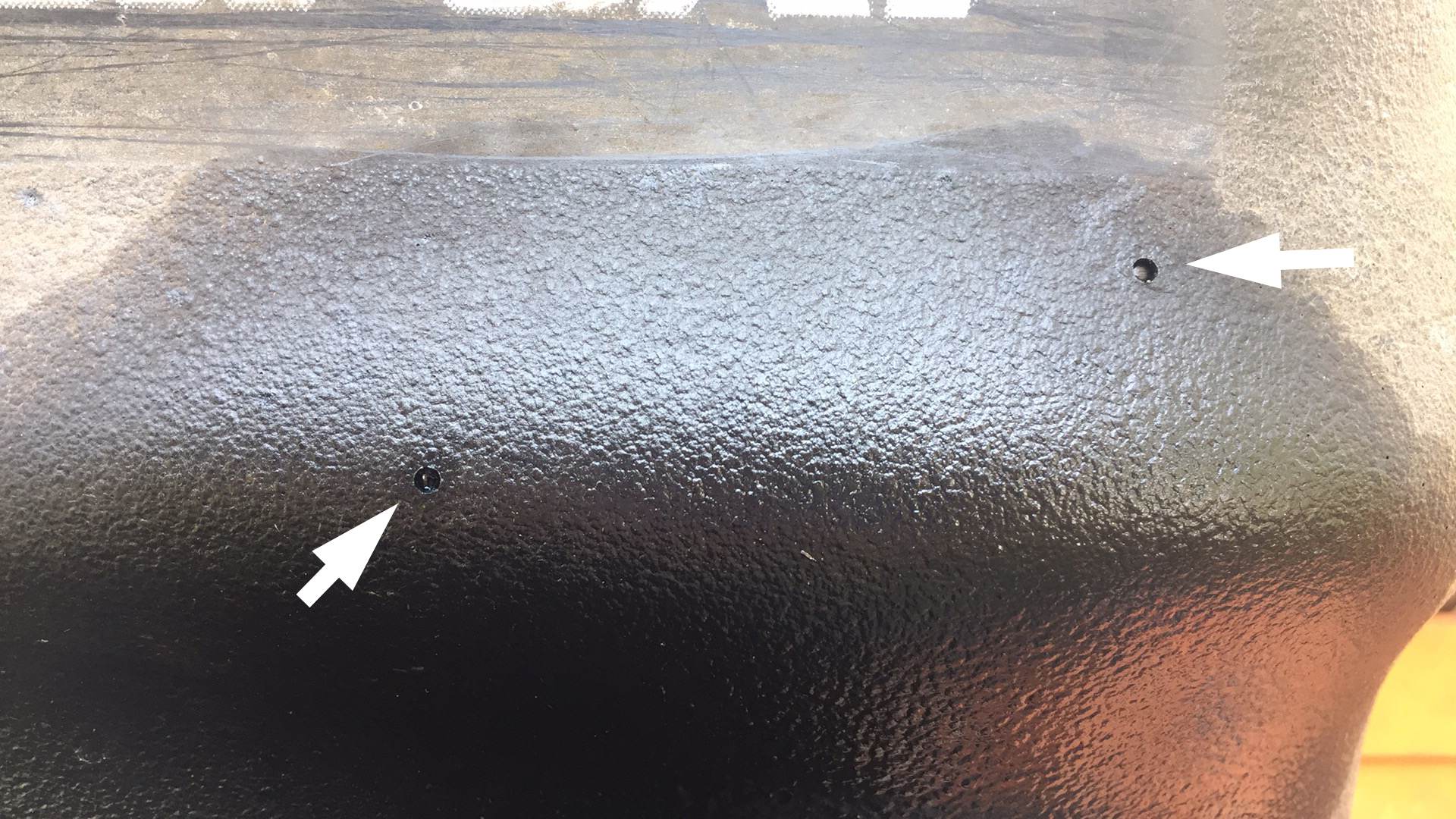
- When working around bats, bites sometimes go unnoticed. Bat bites may be extremely small and generally painless. ANY unprotected physical contact with a live bat puts you at risk for rabies–another good reason for rabies pre-exposure vaccine.
- If you must handle a live bat, use thick leather wildlife gloves.
- If you must enter areas of large bat colonies consider wearing a fit-tested respirator. Rabies is thought to be contracted only through bites; however there is some circumstantial evidence that urine or feces might on occasion be capable of aerial transmission, especially in areas of dense bat numbers.
- If you’ve been bitten recently by a dog or other wildlife and not gotten the post-exposure treatment, consider getting it. Rabies virus can incubate in humans quietly for months after exposure. Although ideally its best to start the shots very soon after the bite, the post exposure prophylaxis can be effective as long as it is given before symptoms appear.
Given that Bonnie and Clyde are still healthy and on the loose in my town, I know now that my emergency room visit and bills last summer were an unnecessary precaution. But if it happened again, I wouldn’t do anything differently, except possibly start my treatment earlier. The risk of rabies is nothing to take lightly, and also I feel better knowing that I have a pre-exposure protection to a very serious health risk.
Animals at risk for rabies
Rabies is found only in mammals, especially carnivores and bats. Animals that can and do get rabies include:
- Skunks are among the highest risk mammals, especially in the south.
- Raccoons are the most commonly infected wild animal in the eastern U.S.
- Bats, have low levels of infection throughout the U.S.
- Foxes, especially in the Southwest and eastern U.S. may be infected with rabies
- Coyotes, are infected in rare cases
- Unvaccinated dogs and cats can be infected with rabies. According to the CDC, dogs are responsible for 90% of human rabies exposures and 99% of human deaths from rabies worldwide.
Rodents and rabbits rarely get rabies–the woodchuck, Marmota monax, a rodent, is an exception. Other low risk animals include oppossums, armadillos, shrews, and prairie dogs. Livestock and horses can get rabies, and because of their close association with humans vaccination is recommended.



















{kind=link}